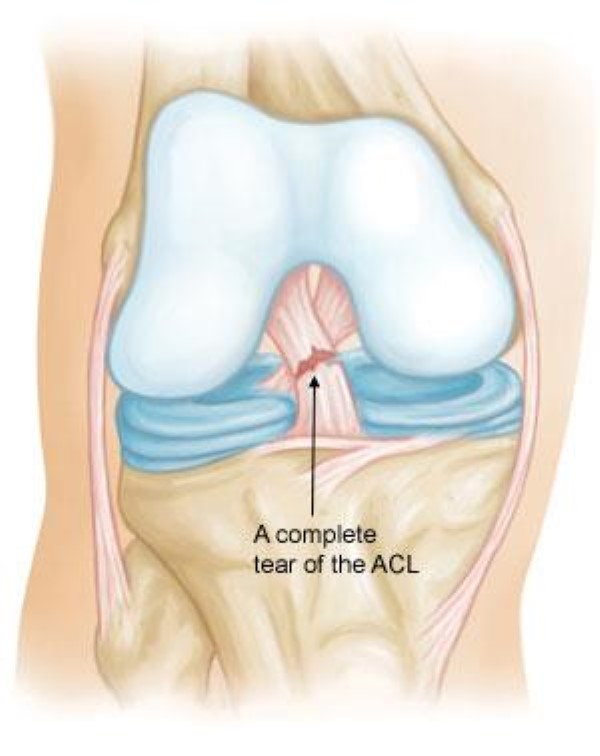
The anterior cruciate ligament (ACL) of the knee is a connective tissue that keeps the knee joint from excessively twisting and gliding forward. This can be damaged or ruptured when the knee receives increased load, more commonly in a pivoting and extended position. Movements such as changing direction and landing in sports of netball, basketball or football are all high-risk positions.
What happens to the body when an ACL is ruptured?
The body relies on the ACL for both knee stability and neuromuscular control. When an ACL is ruptured, the Tibia can glide forward and is able to have increased twist or laxity. This disrupts the biomechanics of the knee, frequently causing giving way and potential knee pain. Having strong muscles around the knee helps this. The ACL also sends signals to the brain of tension and joint position. When this is ruptured, the signal is lost and things like balance and movement patterns are disrupted. Evidence suggests that this disruption has be recorded for up to 3 years.
Current recommendations:
In Australia approximately 70% of ACL ruptures undergo surgery to reconstruct the ligament. This rate is much lower in some other countries.
Currently literature suggests that there is a lack of evidence to recommend surgical intervention for acute ACL injuries. However, recent evidence suggests that chronic ACL injuries have substantial long-term benefits to immediately undergo surgery before undergoing rehabilitation.
What’s involved in surgery?
Surgery generally consists of the formation of a new ACL with the use of a hamstring graft, or more rarely an adductor, patella tendon or quadriceps graft. This new ACL is then surgically connected in place of the old ACL. In recent procedures, some surgeons are opting for the further Iliotibial band (ITB) separation and reconnection to further stabilise the knee joint.
Post surgical rehabilitation:
Rehabilitation is often guided by a physiotherapist with the use of an evidence-based protocol. Generally, the main aim for the initial two weeks is to maximise range of the joint with passive movements and active stretches to reach greater range of the knee joint. Throughout the first 6 weeks, all exercises and movements must follow a restrictive activity guide to ensure reduced risk of rupture. These restrictions include the absence of running, jumping, twisting, open kinetic chain exercise, and deep squatting. From this stage, various exercises will be progressed to optimise walking gait pattern and eventually move towards strengthening, running and return to sport. The risks of tearing the ACL of the opposite side are increased dramatically for the first 12 weeks of rehab.
Conservative Rehabilitation:
When it comes to rehabilitating a knee conservatively with a ruptured ACL, a strict exercise rehabilitation program is required. The risks of meniscal damage (Cartilage) of the knee are greater when returning to pivoting sports such as football or basketball with this approach. The muscles surrounding the knee as well as all muscles involved in lower limb movement must be strengthened to brace the knee and keep alignment during functional activities. Balance and neuromuscular control are heavily affected and will also be a large part of return to sport rehabilitation.
Have you ever seen how a knee moves with a ruptured ACL?
Check out our ACL video on facebook, instagram @pivotalphysioandpilates or linked in showing laxity of the knee joint.
Both surgery and conservative approach can be beneficial to the function of the knee and is widely up to the individual and their lifestyle goals. Contact us at Pivotal Physiotherapy & Pilates to find out more information or begin your rehab journey.
~ Jacob Spencer, Physiotherapist
References:
Lee JH, Han SB, Park JH, Choi JH, Suh DK, Jang KM. Impaired neuromuscular control up to postoperative 1 year in operated and nonoperated knees after anterior cruciate ligament reconstruction. Medicine (Baltimore). 2019 Apr;98(15):e15124. doi: 10.1097/MD.0000000000015124. PMID: 30985673; PMCID: PMC6485889.
Rodriguez K, Soni M, Joshi PK, Patel SC, Shreya D, Zamora DI, Patel GS, Grossmann I, Sange I. Anterior Cruciate Ligament Injury: Conservative Versus Surgical Treatment. Cureus. 2021 Dec 6;13(12):e20206. doi: 10.7759/cureus.20206. PMID: 35004026; PMCID: PMC8730351.
Saueressig T, Braun T, Steglich N, et al. 2022, Primary surgery versus primary rehabilitation for treating anterior cruciate ligament injuries: a living systematic review and meta-analysis, British Journal of Sports Medicine;56:1241-1251.