[!] Trigger warning—the content of this article may be distressing for some.
As if being pregnant and preparing for a new little person in your life isn’t challenging enough…surely every pregnant woman has heard a library-worth of birth horror stories before she even gets to the third trimester! We have to remind ourselves that well-meaning folks love to share the very best and worst of their own experiences and we seldom hear the majority that fall somewhere in the middle.
That said, as women’s health physiotherapists we’re here to educate, guide and care for you throughout your pregnancy to help minimise any risks; empower you during birth; and to ensure a speedy, thorough recovery.
Perineal tears and Obstetric Anal Sphincter Injuries (OASI)
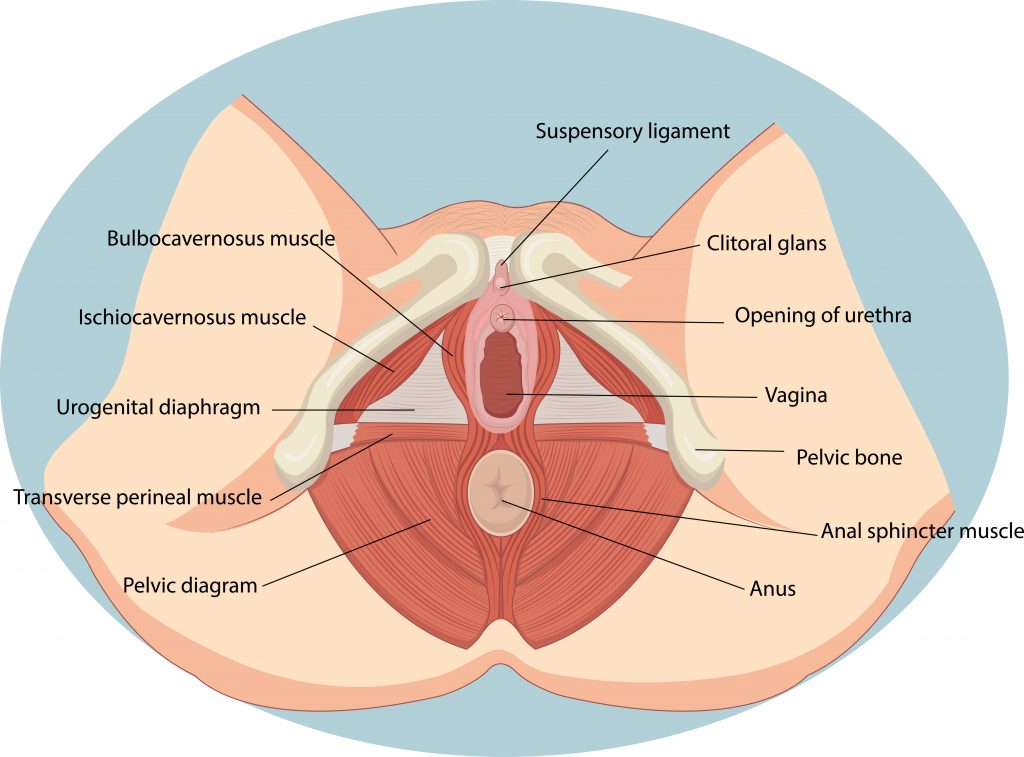
The perineum is a body of connective tissue between your vagina and anus that helps support the floor and organs of the pelvis. Some degree of tearing is common during childbirth, to accommodate the head and body of the baby through the birth canal. It is more common for first time mothers and most tears are only minor and heal quite quickly. There is a classification system used to diagnose perineal lacerations following childbirth, depending on the severity and structures involved. This is when you might hear another mama talk about her “grade X tear”.
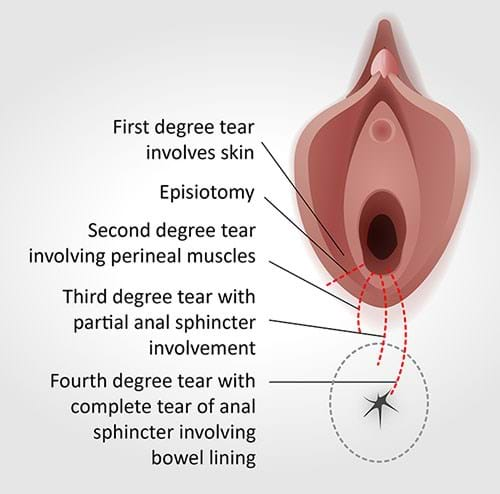
The more severe tears (i.e., grades three and four) are referred to as OASI (or OASIS) because they involve the anal sphincter muscles, which control our wind and bowel movements. In Australia, OASI rates are estimated to be approximately 3% of all vaginal births. However, there’s a significant variation across different states and regions (from 0.6% – 7.1%) because of different factors, including: processes used; access to healthcare; education; and experience.
There are several risk factors that can increase one’s risk of experiencing an OASI, such as:
- Instrumental delivery (particularly forceps)
- Prolonged second stage labour
- Higher maternal age
- First time mothers
- Occipito-posterior position of the baby (back of baby’s head against mother’s spine)
- Large infant head circumference in proportion to a mother’s pelvic cavity
An OASI can bring about the following (manageable) implications:
- Perineal pain
- Incontinence – both urinary and faecal/flatus
- Dyspareunia – pain during sexual intercourse
- Depression/anxiety
In 60-80% of women affected, surgical repair is successful in eliminating symptoms, so it’s important to accurately diagnose the more severe tears to avoid any potential long-term problems. Of course, the earlier, the better.
Pelvic floor and levator ani avulsion
Alongside OASI, pelvic floor muscle trauma and levator ani avulsion are other possible complications in vaginal birth. These are more common and can cause longer-term pelvic floor dysfunction, however there are many ways to reduce the risk.
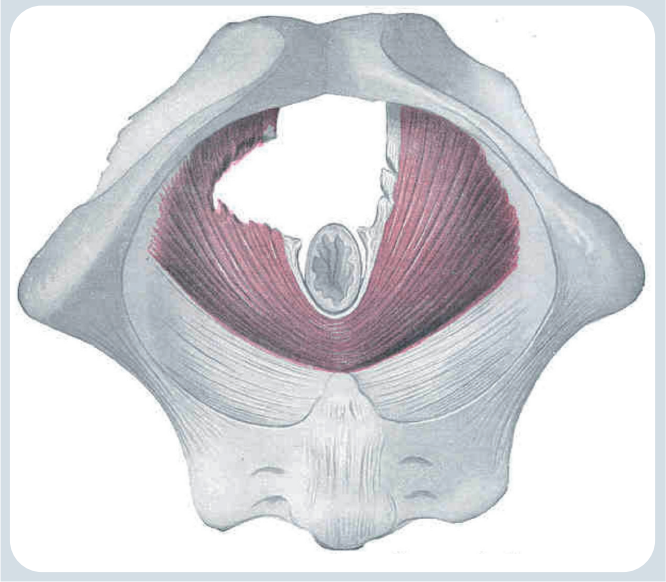
Our levator ani comprises of three muscles that make up part of the pelvic floor. They are key in pelvic organ support as well as maintaining urinary and faecal incontinence. “Levator ani avulsion” refers to when the pelvic floor muscles have detached from the pubic bone in some way.
Think of your pelvic floor muscles like a hammock or sling that lies at the base of our pelvic cavity, supporting our pelvic organs (bladder, uterus, cervix, vagina, and rectum). When we stand, gravity pulls these organs downwards and our pelvic floor muscles keep them in place. During pregnancy, bub creates a lot more weight and force pushing down on these muscles, so they’re having to work extra hard to support our pelvic organs, keep in urine and look after ever-growing bubs. Therefore, it’s so important to strengthen these muscles throughout pregnancy to make sure they can meet the growing demands and support the additional weight, but also to build up endurance for labour.
OASI, together with forceps use and a prolonged second stage of labour, are risk factors associated with levator avulsion. Levator avulsion is also a significant risk factor for the development of pelvic organ prolapse (POP) later in life and recurrence, even after surgical intervention (which involves the insertion of mesh implants).
In part two of this blog, we’ll look at ways to reduce the risk, treat the problem and recover optimally.
~ Sophie Alderslade, Physiotherapist
References
Australian Commission on Safety and Quality in Health Care. Third and Fourth Degree Perineal Tears Clinical Care Standard. Sydney: ACSQHC; 2021.
Australian Commission on Safety and Quality in Health Care (the Commission) 2017, The Second Australian Atlas of Healthcare Variation, Women’s health and maternity, ‘3.5 Third- and fourth-degree perineal tear’, <https://www.safetyandquality.gov.au/sites/default/files/migrated/3.5-Third-and-fourth-degree-perineal-tears.pdf>.
Ducarme, G., Pizzoferrato, A. C., de Tayrac, R., Schantz, C., Thubert, T., Le Ray, C., Riethmuller, D., Verspyck, E., Gachon, B., Pierre, F., Artzner, F., Jacquetin, B., & Fritel, X. 2019, ‘Perineal prevention and protection in obstetrics: CNGOF clinical practice guidelines’, Journal of gynecology obstetrics and human reproduction, 48(7), 455–460, <https://doi.org/10.1016/j.jogoh.2018.12.002>.